THE EUROPEAN DEFINITION OF GENERAL PRACTICE / FAMILY MEDICINE. WONCA EUROPE 2023 Edition
THE EUROPEAN DEFINITION
OF
GENERAL PRACTICE / FAMILY MEDICINE WONCA EUROPE 2023 Edition
THE EUROPEAN DEFINITION OF
GENERAL PRACTICE / FAMILY MEDICINE
WONCA EUROPE 2023 Edition

(Revised 2011 and 2023)
THE EUROPEAN DEFINITIONS of
The Key Features of the Discipline of General Practice
The Role of the General Practitioner
and
A description of the Core Competencies of the General Practitioner / Family Physician. Prepared for WONCA EUROPE (The European Society of General Practice/ Family Medicine), 2002.
Dr Justin Allen
Director of Postgraduate General Practice Education Centre for Postgraduate Medical Education, University of Leicester, United Kingdom
President of EURACT
Professor Bernard Gay
President, CNGE, Paris, France University of Bordeaux, France
Professor Harry Crebolder
Maastricht University The Netherlands
Professor Jan Heyrman
Catholic University of Leuven, Belgium
Professor Igor Svab
University of Ljubljana, Slovenia
Dr Paul Ram
Maastricht University The Netherlands
Edited by:
Dr Philip Evans
President WONCA Europe
This statement was published with the support and co-operation of the WHO Europe Ofce, Barcelona, Spain.
Revised in 2005 by a working party of EURACT Council led by Dr Justin Allen, on behalf of WONCA European Council.
Revised in 2011 by a Commission of the WONCA European Council led by Dr. Ernesto Mola and Dr. Tina Eriksson
Revised in 2023 by a Commission of the WONCA European Council led by Professor Adam Windak, Dr. Andrée Rochfort and Dr. Jean-Pierre Jacquet
Design and Layout: Gözde Usgurlu (gozde@uskur.com.tr)
Table of Contents
1. INTRODUCTION TO THE 2002 EDITION 4 INTRODUCTION TO 2023 REVISION 5 INTRODUCTION TO 2011 REVISION 6 INTRODUCTION TO 2005 REVISION 6
2. THE EUROPEAN DEFINITIONS 2023 7 THE DISCIPLINE AND SPECIALTY OF GENERAL PRACTICE / FAMILY MEDICINE 7
3. EXPLANATORY NOTES, RATIONALE AND ACADEMIC REVIEW - THE NEW DEFINITIONS 9 3.1 EXPLANATORY NOTES 9 3.2 RATIONALE FOR THE DEFINITIONS - ACADEMIC REVIEW AND ANALYSIS 12
4. EXPLANATORY NOTES, RATIONALE AND ACADEMIC REVIEW – THE CORE COMPETENCIES 22 4.1. EXPLANATORY NOTES 22 4.2 ESSENTIAL APPLICATION FEATURES 24 4.3 IMPLEMENTATION BEDROCK 25 4.4 RATIONALE FOR THE CORE COMPETENCIES; ACADEMIC REVIEW AND ANALYSIS 26
5. APPENDICES 30 Appendix 1 30 Appendix 2 31 Appendix 3 32 Appendix 4 33 Appendix 5 34
Using this document
This document contains statements of the characteristics of the discipline and the core com petences, and then sections with short explanatory notes. This is followed by a full explanation of the rationale, and the supporting academic analysis for each, which is important for those wishing to gain a greater understanding of the rationale for their development.
It provides essential information on the discipline of general practice, which should be used to inform those responsible for delivering health care, developing teaching and learning pro grammes for training, and for those learning our discipline.
A shortened version has also been published which contains only the explanatory notes.
1. INTRODUCTION TO THE 2002 EDITION
This consensus statement defnes both the discipline of general practice / family medicine, and the profes sional tasks of the family doctor; it also describes the core competencies required of general practitioners. It delineates the essential elements of the academic discipline and provides an authoritative view on what family doctors in Europe should be providing in the way of services to patients, in order that patient care is of the highest quality and also cost effective. From the defnitions within this paper the agendas for edu cation, research, quality assurance can be derived, to ensure that family medicine will develop to meet the health care needs of the population in the 21st century.
There are signifcant differences in the way that health care systems are organised and family medicine is practiced throughout Europe. For European Union countries, and those aspiring to join the Union, med
ical education is governed by EU Directive 93/16 which is primarily intended to promote free movement of doctors. Unfortunately within the Directive there is a lack of emphasis on the content and quality of post
graduate training. It is therefore self-evident and of great importance that, for the protection of patients, family doctors should receive training that will equip them with the necessary skills to practice in any mem
ber state.
This statement has been produced on behalf of WON CA Europe (The European Society of General Practice / Family Medicine) the Regional Organisation of the World organisation of Family Doctors (WONCA).
WONCA Europe provides the academic and scientif ic leadership and representation for the discipline of Family Medicine throughout the continent. Its mem bership comprises the national academic organisa tions of Family Medicine from 30 European countries, and direct membership from individual family doctors.
REFERENCE
Its main role is to promote and develop the discipline in order to achieve and maintain high standards of ed ucation, training, research and clinical practice for the beneft of individual patients and communities.
Reform of national health systems is a common feature in Europe as elsewhere in the world. Given the chang es in demography, medical advances, health econom ics, and patients’ needs and expectations new ways of providing and delivering health care are being sought. International evidence1 indicates that health systems based on effective primary care with highly -trained generalist physicians (Family Doctors) practising in the community, provide both more cost effective and more clinically effective care than those with a low pri
mary care orientation.
It is vital that the complex and essential role of Fam ily Doctors within health systems is fully understood within the medical profession, but also by the profes sions allied to medicine, health care planners, econ omists, politicians and the public. Within Europe in creased investment in Family Medicine is required to
enable health systems to fulfl their potential on behalf of patients, investment not just in relation to human resources and infrastructure but with regard to edu cation, research and quality assurance.
These new defnitions and the statement of core com petencies are published in order to inform and to con tribute to the debate on the essential role of family medicine within health systems, at both national and pan –European levels.
Dr Philip Evans, President WONCA Europe, 2002
1. Starfeld B. Primary care: balancing health needs, services and technology. Oxford: Oxford University press,1998
4
INTRODUCTION TO 2023 REVISION
Professor Adam Windak
Dr. Andrée Rochfort
Dr. Jean-Pierre Jacquet
This revision of the European Defnition of General Practice / Family Medicine is necessary in 2023 to highlight the relevance of One Health, Planetary Health and Sustainability to the discipline of GP/FM and to refect the urgency of action that is required by all who work in GP/FM and their leaders and representatives for the critical reason of preparing today for the future of humanity.
‘One Health’ is an integrated, unifying approach to balance and optimize the health of people, all animals and the environment¹
‘Planetary health’ is defined as the health of humans and the natural systems on which human health depends such as water, air and soil, which also impact on plant life, food and energy systems².
The Earth’s natural systems are the foundation of the Sustainable Development Goals³.
We all share the same resources, and we are co-dependent on environmental factors. In recent years we have been made aware of how we as humans contaminate water air and soil during our activities of everyday living, and also when at work in the healthcare sector delivering healthcare to patients, such as when prescribing, re questing medical tests and referring people to other services they must travel to. We are all actively consuming things, ranging from the raw materials themselves (energy, water, fuel) to processed products (e.g. food). We also do this in healthcare and other related activities. As a consequence, we should all be concerned with what resources are consumed to produce these activities, what pollution is generated and what waste is produced. We need to know how we can help our planet not to be damaged as it supplies resources for our modern living environments, and how we can avoid making our planet unhealthy as we humans escalate our consumption of resources. The potential of primary care to positively impact healthcare sustainability and address the impact of climate and natural environment change is substantial. As frontline healthcare workers within their respective communities, primary care providers can advocate for measures to reduce the effects of climate and environ ment change, encourage public participation, and promote activities that safeguard individuals from the conse
quences of these changes⁴.
REFERENCES
1. One Health. World Health Organization.
https://www.who.int/europe/initiatives/one-health
2. WONCA Statement on Planetary Health and Sustainable Development Goals. https://www.globalfamilydoctor.com/news/planetary healthandsustainabledevelopmentgoals.aspx
3. Sustainable Development Goals. United Nations, Department of Economic and Social Affairs https://sdgs.un.org/goals
4. Klemenc Ketiš Z, Rochfort A. Sustainability for Planetary Health: A Seventh Domain of Quality in Primary Care. Zdr Varst. 2022 Sep 28;61(4):198-200.
5
INTRODUCTION TO 2011 REVISION
Dr. Ernesto Mola
Dr. Tina Eriksson
At the meeting of 2010 in Malaga the WONCA Europe Council decided to appoint a small Commission, made up of people from different countries and networks, to make a minor revision of the European Defnition of General Practice in order to include two new concepts: Patient Empowerment and Continuous Quality Improvement.
Following a work plan agreed upon with the Executive Board, the commission examined two systematic propos als, based on a wide range of background knowledge, concerning the inclusion into the defnitions of patient empowerment and of continuous quality improvement.
At the end an amended version of the defnitions (based on the members opinions) was written down and sent to the Colleges in July 2011 to allow for an informed discussion at the subsequent European Council in Warsaw, where it was approved.
“Promotes patient empowerment” has been included as a 12th characteristic of the defnition I and a few sen tences have been added in defnitions II and III and in the explanatory notes.
Concerning Continuous quality improvement there isn’t a new bullet in the frst defnition, because it is not a core characteristic of general practice but of all the disciplines. Few sentences have been changed or added in defnitions II and III and in the explanatory notes.
The minor revision was aimed to update the defnitions and make them more adherent to the reality of general practice and of primary care and to the needs created by social and epidemiological changes.
INTRODUCTION TO 2005 REVISION
Professor Igor Svab, President WONCA Europe 2005
Since the defnition was frst accepted in 2002, it has received a wide attention by family physicians, academics and policymakers. It has been translated in most European languages and has been a basis for family practice curricula and a starting point for negotiating contracts with family physicians in many European countries. It has managed to be relevant to family physicians throughout Europe, regardless the enormous differences in the ways family medicine is practiced and taught.
Nevertheless, there was a feeling that more work should be done in order to improve its clarity, so that it would be more easily understandable. This is the reason why the defnition was revised and a new version created.
The 2005 revision of the document has maintained all the elements of the previous defnition. The defnition still defnes both the discipline of general practice / family medicine, and the professional tasks of the family doctor and describes the core competencies required of general practitioners. All the key features of the discipline and the core competencies have remained the same.
The revised defnition will certainly still be used in many occasions when family medicine is being discussed. It has already become a very useful instrument in negotiations with policymakers, educators, media and physi cians themselves.
WONCA Europe will continue to promote the defnition through its member colleges and the networks.
6
2. THE EUROPEAN DEFINITIONS 2023
THE DISCIPLINE AND SPECIALTY OF
GENERAL PRACTICE / FAMILY MEDICINE
General practice / family medicine is an academic and scientifc discipline, with its own educational content, research, evidence base and clinical activity, and a clinical specialty orientated to primary care.
I. The characteristics of the discipline of general practice/family medicine are that it:
a) is normally the point of frst medical contact within the health care system, providing open and unlimited access to its users, dealing with all health problems re gardless of the age, sex, or any other characteristic of the person concerned.
b) makes efcient use of health care resources through co-ordinating care, working with other professionals in the primary care setting, and by managing the inter face with other specialities taking an advocacy role for the patient when needed.
c) develops a person-centred approach, orientated to the individual, his/her family, and their community.
d) promotes patient empowerment
e) has a unique consultation process, which establish es a relationship over time, through effective commu nication between doctor and patient
f) is responsible for the provision of longitudinal con tinuity of care as determined by the needs of the pa tient.
g) has a specifc decision making process determined by the prevalence and incidence of illness in the com munity.
h) manages simultaneously both acute and chronic health problems of individual patients.
i) manages illness which presents in an undifferentiat ed way at an early stage in its development, which may require urgent intervention.
j) promotes health and wellbeing of patients and the ecosystems they live in both by appropriate and effec tive intervention.
k) has a specifc responsibility for the health of the community and environment.
l) deals with health problems in their physical, psycho logical, social, cultural, environmental and existential dimensions.
II. The Specialty of General Practice / Family Medicine
General practitioners/family doctors are specialist physicians trained in the principles of the discipline. They are personal doctors, primarily responsible for the provision of comprehensive and continuing care to every individual seeking medical care irrespective of age, sex and illness. They care for individuals in the context of their family, their community, their culture and integrated health of the planet, always respecting the autonomy of their patients.
They recognise they will also have a professional re sponsibility to their community and environment. In negotiating management plans with their patients they integrate physical, psychological, social, cultural, existential and planetary health-related factors, utilis ing the knowledge and trust engendered by repeated contacts. General practitioners/family physicians ex ercise their professional role by promoting health, pre venting disease and providing cure, care, or palliation and promoting patient empowerment and self-man agement in regard to the co-benefts of improving in dividual and planetary health. They do this by caring for the ecosystem made up of people, animals and the natural environment, being aware of their unique po sition as a role model for their patients regarding the promotion of leading a sustainable way of life. This is done either directly or through the services of others according to health needs and the resources available within the community they serve, assisting patients where necessary in accessing these services. They must take the responsibility for developing and main taining their skills, personal balance and values as a basis for effective and safe patient care. Like other medical professionals, they must take responsibility for continuously monitoring, maintaining and if neces sary improving clinical aspects, services and organisa tion, patient safety and patient satisfaction of the care they provide.
.
7
III. The Core Competencies of the General Practition er / Family Doctor
A defnition of the discipline of general practice/family medicine and of the specialist family doctor must lead directly the core competencies of the general practi tioner/family doctor. Core means essential to the dis cipline, irrespective of the health care system in which they are applied.
The twelve central characteristics that defne the dis cipline relate to twelve abilities that every specialist family doctor should master. They can be clustered into six core competencies (with reference to the characteristics):
1. Primary care management (a,b)
2. Person-centred care (c,d,e,f)
3. Specifc problem solving skills (g,h)
4. Comprehensive approach (i,j)
5. Community orientation (k)
6. Holistic modelling (l)
Particularly in reference to the competencies 1. and 3. quality improvement must be considered included as a fundamental ability.
As a person-centred scientifc discipline, three addi tional features should be considered as essential in the application of the core competences:
a. Contextual: Understanding the context of doctors themselves and the environment in which they work, including their working conditions, community, cul ture, fnancial and regulatory frameworks.
b. Attitudinal: based on the doctor’s professional capa bilities, values and ethics
c. Scientifc: adopting a critical and research based approach to practice and maintaining this through continuing learning and quality improvement
One Health, Planetary Health and Sustainability create the bedrock, allowing a new integrated approach to all of the six core competencies, twelve characteristics and three additional features essential in their application.
8
3. EXPLANATORY NOTES, RATIONALE AND ACADEMIC REVIEW - THE NEW DEFINITIONS
3.1 EXPLANATORY NOTES
The Discipline and Specialty of General Practice/Family Medicine
There is a need to defne both the discipline of general practice/family medicine and the role of the specialist family doctor. The former is required to defne the academic foundation and framework on which the discipline is built, and thus to inform the development of education, research, and quality improvement. The latter is need ed to translate this academic defnition into the reality of the specialist family doctor, working with patients in health care systems throughout Europe.
3.1.1 The characteristics of the discipline of general practice/family medicine are that it:
a) is normally the point of frst medical contact within the health care system, providing open and unlimited access to its users, dealing with all health problems regardless of the age, sex, or any other characteristic of the person concerned
“Normally” is used to indicate that in some circum stances, e.g. major trauma, it is not the frst point of contact. However it should be the point of frst con tact in most other situations. There should be no bar riers to access, and family doctors should deal with all types of patient, young or old, male or female, and their health problems. General practice is the essential and the frst resource. It covers a large feld of activities determined by the needs and wants of patients. This outlook gives rise to the many facets of the discipline and the opportunity of their use in the management of individual and community problems.
b) makes efcient use of health care resources through co-ordinating care, working with other professionals in the primary care setting, and by managing the inter face with other specialities taking an advocacy role for the patient when needed...
This coordinating role is a key feature of the cost ef fectiveness of good quality primary care ensuring that patients see the most appropriate health care profes sional for their particular problem. The synthesis of the different care providers, the appropriate distribu tion of information, and the arrangements for ordering treatments rely on the existence of a coordinating unit. General practice can fll this pivotal role if the struc tural conditions allow it. Developing team work around the patient with all health professionals will beneft the quality of care. By managing the interface with other
specialties the discipline ensures that those requiring high technology services based on secondary care can access them appropriately. A key role for the discipline is to provide advocacy, protecting patients from the harm which may ensue through unnecessary screen ing, testing, and treatment, and also guiding them through the complexities of the health care system.
The discipline recognizes the responsibility to mon itor and systematically assess the quality and safety, in a range of aspects of the care delivered by GPs and practices, followed by action aimed also at improving quality.
c) develops a person-centred approach, orientated to the individual, his/her family, and their community.
Family medicine deals with people and their problems in the context of their life circumstances, not with im personal pathology or “cases”. The starting point of the process is the patient. It is as important to understand how the patient copes with and views their illness as dealing with the disease process itself. The common denominator is the person with their beliefs, fears, ex
pectations and needs.
d) promotes patient empowerment
Family medicine is in a strategic position to promote the goals of patient empowerment and self manage ment. Longitudinal care, a multidisciplinary approach, a strong relationship based on a unique consultation process and on trust, a person-centred approach, are the starting points for a continuous educational pro
cess aimed to empower the patient.
9
e) has a unique consultation process, which establish es a relationship over time, through effective commu nication between doctor and patient
Each contact between patient and their family doctor contributes to an evolving story, and each individual consultation can draw on this prior shared experience. The value of this personal relationship is determined by the communication skills of the family doctor and is in itself therapeutic.
f) is responsible for the provision of longitudinal con tinuity of care as determined by the needs of the pa tient.
The approach of general practice must be constant from birth (and sometimes before) until death (and sometimes afterwards). It ensures the continuity of care by following patients through the whole of their life. The medical fle is the explicit proof of this con stancy. It is the objective memory of the consultations, but only part of the common doctor-patient history. Family doctors will provide care over substantial pe
riods of their patients’ lives, through many episodes of illness. They are also responsible for ensuring that healthcare is provided throughout the 24 hours, com missioning and coordinating such care when they are unable to provide it personally.
g) has a specifc decision making process determined by the prevalence and incidence of illness in the com munity.
Problems are presented to family doctors in the com munity in a very different way from the presentations in secondary care. The prevalence and incidence of illnesses is different from that which appears in a hospital setting and serious disease presents less fre quently in general practice than in hospital because there is no prior selection. This requires a specifc probability based decision-making process which is informed by a knowledge of patients and the commu nity. The predictive value, positive or negative of a clin ical sign or of a diagnostic test has a different weight in family medicine compared to the hospital setting. Frequently family doctors have to reassure those with anxieties about illness having frst determined that such illness is not present.
h) manages simultaneously both acute and chronic health problems of individual patients.
Family medicine must deal with all of the health care problems of the individual patient. It cannot lim it itself to the management of the presenting illness alone, and often the doctor will have to manage mul tiple problems. The patient often consults for sever al complaints, the number increasing with age. The simultaneous response to several demands renders necessary a hierarchical management of the problems which takes account of both the patient’s and the doc tor’s priorities.
i) manages illness which presents in an undifferenti ated way at an early stage in its development, which may require urgent intervention.
The patient often comes at the onset of symptoms, and it is difcult to make a diagnosis at this early stage. This manner of presentation means that important decisions for patients have to be taken on the basis of limited information and the predictive value of clin ical examination and tests is less certain. Even if the signs of a particular disease are generally well known, this does not apply for the early signs, which are often non-specifc and common to a lot of diseases. Risk management under these circumstances is a key fea ture of the discipline. Having excluded an immediate
ly serious outcome, the decision may well be to await further developments and review later. The result of a single consultation often stays on the level of one or several symptoms, sometimes an idea of a disease, rarely a full diagnosis.
j) promotes health and well being of patients and the ecosystems they live in both by appropriate and effec tive intervention.
Interventions must be appropriate, effective and based on sound evidence whenever possible. Intervention when none is required may cause harm, and wastes valuable health care resources. Interventions should take into account the well-being not only of individu als, but also of living (fora and fauna) and non-living (climate, air, water, soil/earth, food, etc.) components of the surrounding ecosystems.
10
k) has a specifc responsibility for the health of the community and environment.
The discipline recognises that it has a responsibility both to the individual patient and to the wider com munity in dealing with health care issues. This ap proach includes integrated health of people, animals and environment, known as the One Health concept. On occasions this will produce a tension and can lead to conficts of interest, which must be appropriately managed.
l)deals with health problems in their physical, psycho logical, social, cultural, environmental and existential dimensions.
The discipline has to recognise all these dimensions si multaneously, and to give appropriate weight to each. Illness behaviour and patterns of disease are varied by many of these issues and much unhappiness is caused by interventions which do not address the root cause of the problem for the patient.
3.1.2 The Specialty of General Practice/ Family Med icine
General practitioners/family doctors are specialist phy sicians trained in the principles of the discipline. They are personal doctors, primarily responsible for the pro vision of comprehensive and continuing care to every
individual seeking medical care irrespective of age, sex and illness. They care for individuals in the context of their family, their community, their culture and envi ronment they live in, always respecting the autonomy of their patients. They recognise they will also have a professional responsibility to their community. In ne gotiating management plans with their patients they integrate physical, psychological, social, cultural and existential factors, utilising the knowledge and trust en gendered by repeated contacts. General practitioners/ family physicians exercise their professional role by pro
moting health, preventing disease, providing cure, care, or palliation and promoting patient empowerment and self-management. They do this caring for One Health, Planetary Health and Sustainable Development Goals. This is done either directly or through the services of others according to their health needs and resources available within the community they serve, assisting patients where necessary in accessing these services. They must take the responsibility for developing and maintaining their skills, personal balance and values as a basis for effective and safe patient care.
This defnition of the role of the family doctor puts the characteristics of the discipline described above into the context of the practising physician. It represents an ideal to which all family doctors can aspire. Some of the elements in this defnition are not unique to family doctors but are generally applicable to the profession as a whole. The speciality of general practice/family medicine is nevertheless the only one which can im plement all of these features. An example of a com mon responsibility is that of maintaining skills, which may be a particular difculty for family doctors who often work in isolation.
11
3.2 RATIONALE FOR THE DEFINITIONS - ACADEMIC REVIEW AND ANALYSISIntroduction
The Leeuwenhorst group produced its statement “The General Practitioner in Europe” in 1974¹. At that stage general practice/family medicine was in its infancy as a discipline, particularly with regard to its teaching and research base. Almost 30 years later the world has moved on and nowhere has this change been more apparent than in the provision of health care. Gener al practice / family medicine is now well established in all health care systems in Europe and is recognised by health service providers as being of ever increas ing importance. This has been emphasised by WHO Europe in its 1998² framework document, and by the way that in most countries in the former Soviet block general practice/family medicine is being introduced as the basis for their new health care systems.
Society has changed over the last 30 years and there has been an increasing role for the patient as a deter mining factor in health care and its provision. The opin ion of the clinician is no longer regarded as sacrosanct and a new dialogue is emerging between health care consumers and providers. The future family doctor has to be not only aware of this change but to be able to thrive in such an environment. It is important that the discipline of general practice / family medicine con tinues to evolve as the health care systems in which it operates change, and that it responds to the health needs of patients. Family doctors must be involved in the continuing development of their health care sys tem, and as individuals must be able to change in order to meet these new challenges.
Van Weel, in his recent lecture to the RCGP Spring Meeting³, emphasised the need for academic develop ment to enable transfer of knowledge, expertise and experience, to develop techniques and methodology addressing the specifc requirements of general prac tice, and to explore the effectiveness of general prac tice care. He also emphasised the importance of the value basis of family medicine itself and the need for a common culture of teaching, research and training. It is timely therefore to re-examine the defnitions of the role of the family doctor, and to develop a clear state ment of the characteristics of the discipline of general practice/family medicine.
There is a further imperative for European Union coun tries, and those aspiring to join the Union. EU Direc tive 93/16⁴ is intended to promote free movement of doctors, and therefore, for the protection of patients, it is self-evident that family doctors should receive training that will equip them with the necessary skills to practice in any member state, as their qualifcation entitles them to practice anywhere in the EU without further training. It follows that it is important to have a consensus view defning the characteristics of the discipline and the tasks that family doctors should do.
Directive 93/16 only defnes a training period of mini mum of 2 years and a minimum of six months in a gen eral practice setting; this has been lengthened to 3 or more years by some countries. The UEMO Consensus document of 1994 on specifc training for general prac tice⁵ argued the need to prolong the period of training to a minimum duration of 3 years including a practical and theoretical part, of which a minimum of 50% of clinical training time must be spent in a general prac tice environment. The Advisory Committee on Medical Training (ACMT)⁶ accepted the views of UEMO and ad vised the European Commission to revise the Directive accordingly - to establish a training period of 3 years, 50% to be located in practice, and general practition ers to be involved and responsible for general practice training at all levels. However unfortunately this advice has not yet been accepted by the European Commis sion.
Problems with bringing about change to Title 4 of the medical directive, which relates to general practice/ family medicine and the need to develop the place of family medicine within the curriculum of medical uni versities have led to the suggestion that further de velopments in the discipline could be better achieved if “specialist in family medicine” became one of the medical specialties listed in Title 3 - which covers all of other medical specialties. It is not part of this paper to explore this issue; the purpose here is to elaborate the principles that underpin the discipline of general practice/family medicine.
12
ROLE, DISCIPLINE AND HEALTH CARE SYSTEM
There are different ways of approaching the problem of producing a new defnition. The method used by the Leeuwenhorst group, and more recently by Olesen et al⁷, was to defne the parameters of the discipline by describing the types of tasks that a family doctor has to carry out. An alternative approach is to try to defne the fundamental principles of the discipline of general practice/family medicine. This approach has been tak en by Gay in a presentation to the inaugural meeting of WONCA Europe in Strasbourg in 1995⁸ and was also
used in the framework document developed by WHO Europe.
Gay has suggested that there is a relationship between principles and tasks with some infuences on the task required from both the patients and the health care system. This should then lead to defnitions of com
petence which will determine the content of general practice education. This is represented in fgure 1.
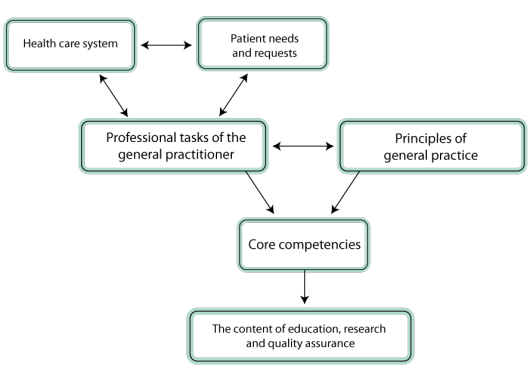
Figure 1 - Relationship between the principles of the discipline of general practice and the tasks demanded of family doctors
13
This diagram indicates the dynamic relationship be tween the underlying principles of the discipline and the tasks that family doctors have to perform. These tasks are determined to a considerable extent by the health care system in which GPs work and the chang ing needs and demands of the patients.
The characteristics as described by WHO Europe, can also be considered as the aims for general practice within the health care system. These concepts bring into play ideas of effectiveness and if one accepts that the health care system determines to a greater or less
er extent the task that a family doctor is able to under take, any new defnition must take into account the context in which the family doctor works and refect the changing needs of patients and advances in health care delivery.
These approaches are not mutually exclusive and any new defnitions will have to take into account the un derpinning principles of the discipline, the core tasks of the family doctor within the health care system and the infuence of the health care system on the provi sion of family medicine.
The principles of the discipline as suggested by Gay were: -
1. Patient centred approach
2. Orientation on family and community context
3. Field of activities determined by patient needs and requests
4. Unselected and complex health problems 5. Low incidence of serious diseases
6. Diseases at early stage
7. Simultaneous management of multiple complaints and pathologies
8. Continuing management
9. Coordinated care
10. Efciency
and are in many ways similar to the characteristics of general practice/family medicine described in the WHO framework statement: -
A. General
B. Continuous
C. Comprehensive
D. Co-ordinated
E. Collaborative
F. Family orientated
G. Community orientated
14
The WHO statement goes on to elaborate what it means by these 7 characteristics.
General: -
• Unselected health problems of the whole population
• Does not exclude categories because of age, sex, class, race or religion, nor any category of health problem
• Easy access, unlimited by geographical, cultural, administrative or fnancial barriers
Continuous: -
• Person centred
• Longitudinal health care, over substantial periods of life, not limited to one illness episode
Comprehensive:-
integrated care involving
• Health promotion, disease prevention, curative, rehabilitative and supportive care • Physical, psychological and social perspectives
• Clinical, humanistic and ethical aspects of the doctor – patient relationship
Co-ordinated: -
• Care managed at frst contact
• Referral to specialist services
• Providing information to patients on available services
• Co-ordinate and manage care
Collaborative: -
• Working in multidisciplinary teams
• Delegating care where appropriate
• Exercising leadership
Family oriented care:-
addressing individual problems in the context of
• Family circumstances
• Social and cultural networks
• Work and home circumstances
Community orientated: -
suggests that family doctors should consider individual problems in the context of: - • The health needs of the community
• Other professionals and agencies
15
WONCA in its 1991 statement on the Role of the General Practitioner/Family Physician in Health Care Systems⁹, produced a defnition of the general practitioner role and linked it to features of general practice/family medi cine which it describes under the categories of commitments and specifcations
The WONCA 1991 statement includes the following
▶ Comprehensive care
▶ Orientation to the patient
▶ Family focus
▶ Doctor/patient relationship
▶ Co-ordination with other services
▶ Advocacy
▶ Accessibility and resource management.
There is a great overlap in the WHO characteristics, the “specifcations” in the WONCA document and in the prin ciples as defned by Gay. This can be demonstrated by cross- mapping them as in the following table:
|
WHO 1998 |
WONCA 1991 |
“Principles” as described by Gay |
|
General |
Comprehensive care |
3. Field of activities determined by patient needs and requests 4. Unselected and complex health prob lems |
|
Continuous* |
Orientation to the patient |
1. Patient centred approach 8. Continuing management |
|
Comprehensive |
Comprehensive care |
3. Field of activities determined by patient needs and requests 4. Unselected and complex health problems |
|
Co-ordinated |
Co-ordination with other services |
9. Coordinated care |
|
Collaborative |
Co-ordination with other services |
9. Coordinated care |
|
Family oriented |
Family focus |
2. Orientation on family and community con text |
|
Community oriented |
Commitment to the Community |
2. Orientation on family and community con text |
* Confusion in the use of language in the WHO document may cause some difcul
ty. The confusion is between the words “continuous”, and “continuing” and in the
context of the WHO document “continuing” would be more appropriate.
Continuous - means without a break; uninterrupted; such as the perimeter fence
around a prison.
16
However there are some interesting differences. The items described by WHO and WONCA are dealing with professional activity in the health care system and not the discipline as a medical activity with a specifc pro
cess. Indeed, the 3 following items concern the disci pline and are not really integrated in the WHO or WON CA characteristics.
“Low prevalence of serious diseases”, “diseases at ear ly stage”, and “simultaneous management of multiple complaints and pathologies” in Gay’s presentation are part of the “comprehensive care” in the WONCA paper, but are not covered in the characteristics of WHO. They cover a crucial aspect of general practice – that it is a people based discipline (as opposed to pathology or organ based), and that it is normality orientated (as opposed to the abnormality orientation of secondary care), but that family doctors will also meet and need to manage serious illness at an early and undifferen tiated stage. The statement from WONCA also makes the point that the incidence of illness, and the signs at presentation are very different in primary care from those seen in hospital, where these are usually taught.
The WHO Framework fails to explore in any depth that which must be regarded as the cornerstone of general practice/family medicine, the individual consultation between patient and family doctor. Gay proposed a theoretical model of general practice: a GLOBAL MOD EL, open minded, considering the disease as the result of organic, human and environmental factors. This concept, in which health is a complex framework, is like the bio psychosocial model of Engel: it’s a “holistic” model.
The consultation is included in the WONCA statement, which also describes the need to express problem defnition for patients in both biomedical and human istic terms; that is in physical, psychological and so cial terms. This has its origin in the report of a work ing party of the Royal College of General Practitioners (RCGP)10, and has become so embedded in the thinking of the discipline that it is in danger of being taken for granted.
EEfciency is a further statement by Gay which is not specifcally mentioned in the WHO characteristics. This presumably refers to the cost efciency which is accepted as a characteristic feature of well developed family health care systems. The WONCA statement develops this idea further, suggesting that the family doctor has a role in resource management in health care systems.
The close inter-relationship between the defning principles of the discipline as previously described and the various role descriptions can be seen if one ex amines the latter in some detail. (See appendix 1.) The original Leeuwenhorst defnition appears to have the advantage over the others of having stood the test of
time and being widely accepted. It was very much set in its own time when general practice was a very new discipline with a limited research and education basis and was usually regarded as the branch of the medical profession to which one sank if one was unskilled in all others. It was informed, at least in part, by the job def nition produced by a working party of the Royal College of General Practitioners in 197210, which also seems to have informed the WONCA defnition. It covers many of the characteristics later described in the WHO frame work but put them into the context of day-to-day work in general practice. However it is not sufcient in itself to be the only defnition; it is not comprehensive – for example curative, rehabilitative and supportive care are not specifcally mentioned.
Olesen et al have stated that the original Leeuwen horst defnition is out of date and does not refect the reality of family medicine today. However it would ap pear that much of the detail of the dissatisfaction ex pressed by Olesen et al is because many of those who regard themselves as family doctors are working in healthcare systems in which it is not possible to com ply with all of the characteristics. Thus they drop some of the features that many would regard as key to the work of the family doctor, particularly losing the con cept of the community setting of the discipline and of longitudinal care - continuity. They cite examples such as family doctors working in emergency departments as support for their viewpoint.
The two succeeding defnitions, those of WONCA 1991 and Olesen 2000, still seem to have their roots very much in the Leeuwenhorst defnition. The WONCA 1991 statement appears to have made it much more relevant to different health care systems and incor porates, as has been described, some descriptors of the discipline. In its clinical decision making section it describes the early presentation of undifferentiated clinical problems, the large number of problems which do not ft with standard biomedical diagnoses and the different prevalence of illness and disease within the general practice setting as compared with the sec ondary care setting.
When considering health care systems the model of health care shown in fgure 2 is now generally accept ed11. If we use the defnition of primary care that is used in the introduction – “the setting within a health care system, usually in the patient’s own community in which the frst contact with the health profession
al occurs” – we are brought into a consideration of the context in which the family doctor works. The interfac es between self-care, primary,
secondary and tertiary health
care and the interactions be
tween the various health care
providers in each are important
issues to be considered.
17

There are a number of patterns of primary health care delivery in Europe, with differences in the patient pop ulation dealt with by family doctors, and an increasing number of different health professionals working in primary care in the different health care systems. The contexts in which such family doctors work are very different, but the underlying principles of the discipline should still apply. Obviously some health care systems may not be the most conducive to good family medi cine, and, though such systems are not easily amena
ble to change, we should not be afraid to put forward a view of the ideal model of the health care system which is likely to provide the best health outcomes and cost-efcient care . That is one which is based on high quality Family Medicine. This was one of the main thrusts of the WHO Framework document
The task is to defne that which is the unique activity of the family doctor – the clinical generalist. Family doc tors should through their activities in preventive med icine and health education have an infuence on self care. In some health care systems they infuence the provision of both secondary and tertiary care and may have a facilitating role in co-ordinating appropriate ac cess to these services. In others, narrow specialists also work in a primary care setting, often dealing with problems that in other countries would be managed by family doctors. In some health care systems family doctors, working predominantly in primary care, may have a limited secondary care role.
18
DISCUSSION
Can all these varied statements and defnitions be Can all these varied statements and defnitions be com bined into one defnition? Do we need a new defnition, and should it be a description of the task/role or of the features of the discipline? This was put to the test in a workshop at the 2001 WONCA Europe Conference in Tampere, Finland, where a substantial majority felt there should be a new defnition, and that it should en
compass a description of both task and the principles of the discipline.
There are many similarities between the statements of the principles which defne our discipline, and in the task descriptions of a general practitioner, but there also signifcant differences. As has been pointed out there are gaps in all the statements, which may be due to differences in the way in which the statements are interpreted. None of these defnitions per se encom pass all the key features of the discipline of general practice. There is therefore a need for a synthesis of the various statements considered thus far to examine the differences, fll the gaps and ensure completeness
Much of the concern regarding the Leeuwenhorst def nition Olesen et al expressed in their paper appears to be in its interpretation in absolute terms. For example what is meant by personal care? Is it care by the same doctor on every occasion? If not what are the condi tions when it is acceptable for a deputy – e.g. out of working hours. Or do we mean care for people rather than pathology – the person orientation of care de scribed by Gay and the WHO? Again the Tampere work shop was consulted on this; very few participants felt that GPs should be providing 24-hour personal care, but a substantial majority felt that they should provide continuing personal care over a substantial period of time.
When we come to consider our defnitions there are a number of other issues that must be emphasised. The unique interaction between family doctor and pa tient that is the general practice consultation merits further exploration. This has been described as a cov enant by McWhinney12, which has its own therapeutic effect. This relationship between doctor and patient in general practice caused Balint13 to coin the term “the drug doctor”. Using the consultation interaction as a therapeutic tool must be regarded as a key feature of general practice and must be part of its training. Perei
ra-Gray14 has further explored the issue of continuity and the use of time by considering the separate con sultations between the GP and the patient over time as part of a continuum. He noted that the average citizen in the United Kingdom consults their GP fve times per year making a cumulative time of 47 minutes per an
num.
An area of increasing importance over recent years has been the concept of patient autonomy and with it the role of the family doctor in developing the expertise of patients in managing their own illness, and contribut
ing to this management by changing behaviour. Em powering patients is a relevant task of general practice by promoting a continuous educational process aimed to increase their self-awareness necessary to effec tively assume responsibility for their health-related decisions15. A patient-empowerment approach re quires that patients’ perspectives regarding their con ditions, their goals, expectations, and needs are the focus of the treatment goals and management activ ities16. This is likely to become increasingly important as patients become better informed due to the wide variety of information systems now becoming available to them, for example the Internet.
Advocacy is featured only in the WONCA statement, al though it was in preliminary drafts of the WHO frame work. It is described as “helping the patient take an active part in the clinical decision-making process and working with the government and other authori ties to maximise equitable distribution of services to all members of society”. There would appear to be a further function of the family doctor, which is about assisting patients negotiate their way around the sec ondary and tertiary parts of their health care systems.
The epidemiology of general practice is essentially different from that of secondary care. Major illness presents early and in an undifferentiated way; many minor, self limiting problems are only or predominant
ly seen in primary care; and family medicine manages much of the longitudinal care of chronic illness. Many consultations are to relieve the anxiety of the possibil ity of illness in patients who have no pathology – the normality orientation of primary care. The concept of normality orientation is complex and covers a number of issues. It encompasses the activity of promoting health and well-being, and the expectation that many of the problems presented to them have no basis in pa thology. At the same time general practitioners must diagnose and manage serious illness, the incidence of which is different co
- Access
- Public
- Year
- 2023